
Radiation Therapy 101
- 5 minute read.
- Last Updated: 1/29/2026
Learn the Basics of Radiation Therapy
Radiation damages the DNA in cancer cells, rendering them unable to reproduce, which hastens their death. The goal in radiation treatment planning is to deliver the most effective dose of radiation to ultimately kill the tumor or tumors, while depositing the least amount of radiation into the surrounding tissues and organs. No matter the dose, in external beam radiation therapy (EBRT), radiation is carried by a beam that travels a path through the body, depositing radiation along the way.
External Beam Radiation Therapy
In conventional EBRT, radiation is carried by a photon beam (neutral/no electromagnetic charge). It enters the body, deposits a maximum radiation dose (dmax) at a shallow depth (around 1.5cm), continues the path to reach the tumor, and continues the path on the other side of the tumor until it exits the body. Once it has delivered the dmax, photons continue to deposit radiation in decreasing amounts along the entire path until exiting the body. In order to spread out the entrance dose, before hitting the tumor, the prescribed dose of radiation is delivered by a series of beams in an arc around the body. This distributes a lesser amount of radiation from each beam, converging on the tumor (the isocenter) so that the tumor receives the large amount of radiation needed to kill the cancer. This method also allows for the beams to be turned off, or decreased, when the beams in the arc pass through a critical organ or structure in their path. The dose of radiation needed to converge on the tumor is still the same, though; so if passing over an organ decreases the dose being delivered, then it has to be made up for on either side of the organ. This is what determines the irregular shape of the target treatment area. EBRT at Thompson is delivered by Gamma Knife, IMRT, or VMAT.

Proton Therapy
Proton therapy, another form of EBRT, also delivers radiation to the tumor, but there are a few things that make it different from photon radiation. Because protons are positively charged particles, they can be designed to release their maximum dose when they reach the tumor, a depth where they achieve a property unique to protons called the Bragg peak. At the Bragg peak, protons dump the bulk of their energy, or radiation, then they stop. They do not continue depositing radiation on a path out of the body on the other side of the tumor, so no exit dose. Instead of using multiple beams to create irregular shapes of radiation, protons can match the shape of the tumor using a single beam. Because protons, again, are positively charged particles, they can be “programmed” to “paint” the tumor, a process called pencil beam scanning. Similar to photon therapy, proton therapy can use multiple beams to “smear” the entrance dose. But, because there is no exit dose, protons can use only 2-3 different beams, instead of an arc. Learn more about Proton Therapy by visiting the Covenant Health Proton Center website.
With all forms of radiation therapy, tissues surrounding the tumor receive radiation, in addition to the radiation deposited along the beam’s path. This is called “dose spill.” Treatment planning intentionally includes an area of volume that surrounds the tumor to receive radiation dose to ensure that the entire irregularly shaped cluster of cancer cells is treated. The treatment plan, telling the radiation where to go, is calculated in such a way as to minimize the radiation delivered to healthy tissues, while maximizing the effective dose to the treatment area. This is called “optimization.”
Each mode of delivery of radiation that Thompson Cancer Survival Center offers has unique properties that makes it shine in treating different cancers. One physicist explained the differences in delivery modes by drawing a dartboard target. He drew a dot right on the bullseye, and said, “That is accurate.” He drew another pair of dots between the bullseye and the smallest ring: “That is precise, but not accurate. It still gets points that can win the game.”
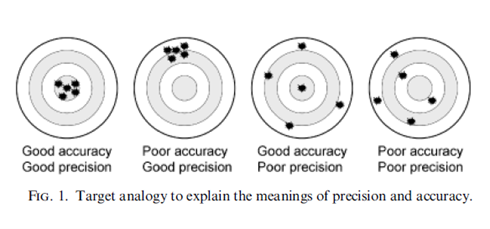
Although this issue is going to explore each radiation option Thompson offers more thoroughly, here is a basic snapshot of their main distinguishing features, keeping the dartboard in mind:
• Gamma Knife is primarily for cranial tumors, nerves and vessels (although it can be used elsewhere in the body, too.) It is possibly the most precise and accurate form of radiation, meaning it shines when treating very small tumors or structures.
• Photon radiation delivered by a linear accelerator (IMRT and VMAT) is also precise, but not as precise as the Gamma Knife. It is highly accurate, though. It shines when you want to treat tumors that are a little bigger, where there are areas that contain multiple tumors, or when treating areas that may experience more movement (for example, with the motion of breathing.)
• Proton therapy is not only accurate, but it is also conformal, and the dose stops inside the tumor, sparing surrounding healthy organs. If the tumor abuts a critical structure in the body that is especially susceptible to damage from radiation, such as the spinal cord, or has received radiation dose previously, the beam can be optimized to enter the body from an angle that hits the tumor and then stops before delivering high doses of radiation to that critical structure
No matter the type of cancer, if the treatment includes radiation therapy, Thompson Cancer Survival Center has all of the technological offerings of the major cancer centers, as well as a superior radiation oncology team of groundbreaking innovators, researchers and clinicians.
Visit our website to learn more.
